Regulatory and Health Industry
What You Need to Know About OIG Audits
Since it was established in 1976, the Office of Inspector General (OIG) has provided objective, independent oversight of the US Department of Health and Human Services (HHS) and has led efforts to fight waste, fraud, and abuse. HHS is the largest civilian agency in the federal government. With a fiscal year 2021 budget of $419 million and 1,600 employees, the OIG conducts nationwide investigations, inspections, and audits that can result in criminal convictions, civil penalties and settlements, and administrative sanctions against those who commit fraud. The OIG uses risk assessments and data analysis to determine emerging issues where they need to implement oversight and enforcement resources.
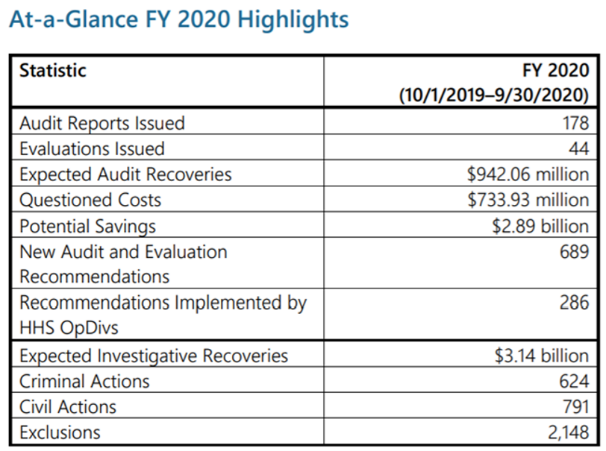
The OIG generates a semiannual report to Congress on the activities of the office. The fall 2020 semiannual report for April 2020 to September 2020 shows that the OIG expects to recover $942.06 million due to audits and $3.14 billion due to investigative recoveries.
{kind=link}
Source: https://oig.hhs.gov/reports-and-publications/archives/semiannual/2020/2020-fall-sar.pdf
Every month, the OIG updates its vigorous work plan to identify and respond to developing issues. The OIG Work Plan outlines all recently added work plan items, active work plan items, and items that have been archived from the work plan. As health information (HI) professionals, it’s important that we continuously monitor the OIG Work Plan to remain current on the plan’s focus areas and determine if we need to perform risk analysis or audits, and/or provide in-depth education to our coding professionals and providers within our organization.
This article highlights a few key focus areas from the active OIG Work Plan. For a complete listing of all active work plan items, see the OIG website.
Documentation Audits
The OIG recently performed an audit to determine if hospitals complied with Medicare billing requirements when assigning an ICD-10-CM diagnosis code for severe malnutrition on inpatient hospital claims. The OIG reviewed $3.4 billion in Medicare payments for 224,175 claims with a discharge date in fiscal year 2016 or 2017 that contained a severe malnutrition ICD-10-CM diagnosis code of E41 or E43 and severe malnutrition was the only major complication or comorbidity (MCC) coded on the account. The deletion of the single MCC from the account would impact the Medicare severity diagnosis-related group (MS-DRG) payment. From these 224,175 claims, the OIG selected 200 accounts for a random audit to determine if severe malnutrition met medical necessity and was properly coded. From the 200 accounts in the random audit, the OIG determined 164 claims were billed incorrectly.
The OIG final report, released July 2020, stated “The hospitals used severe malnutrition diagnosis codes when they should have used codes for other forms of malnutrition or no malnutrition diagnosis code at all, resulting in net overpayments of $914,128. Based on our sample results, we estimated that hospitals received overpayments of $1 billion for FYs 2016 and 2017.” The OIG found similar issues with the coding of malnutrition in earlier audits for years 2016, 2017, and 2018.
Anytime there is only one MCC/complication or comorbidity (CC) condition coded on the account, you need to ensure there is documentation that clearly supports the condition. Does the condition meet the Uniform Hospital Discharge Data Set (UHDDS) definition for Other Diagnoses? UHDDS defines other diagnosis as “all conditions that coexist at the time of admission, that develop subsequently, or that affect the treatment received and/or the length of stay.” The ICD-10-CM guidelines state that diagnosis codes can be assigned for additional conditions if those conditions affect patient care in terms of requiring clinical evaluation; therapeutic treatment; diagnostic procedures; extending the length of the hospital stay; or increasing nursing care and/or monitoring.
What follows are a few key questions for you to consider as you determine if your facility is vulnerable to an OIG investigation surrounding the diagnosis of malnutrition.
- Have you analyzed your organization’s data to see if there are any coding trends for malnutrition?
- Do you have an internal audit plan in place to verify if this diagnosis is coded and documented correctly?
- Do you see a significant trend of accounts where malnutrition is the only MCC/CC coded on the account?
- Are you receiving high denial rates from Medicare or other insurance companies on the diagnosis of severe malnutrition?
- Have you provided education to your coding, clinical documentation team, and providers on the coding and billing of malnutrition?
If you and/or your facility bills for inpatient facility accounts, these are all questions to answer to determine if your facility is at risk for an OIG malnutrition audit.
Facet Joint Injections
Facet joint injections are an interventional technique used to diagnose or treat back pain. Several previous reviews found significant billing errors in this area, including a prior OIG review. As of August 2019, the OIG has added facet joint injections as an active work plan item. The OIG will review whether payments made by Medicare for facet joint procedures billed by physicians complied with federal requirements.
Understanding spinal anatomy is the first step to ensuring reimbursement through correct coding. Most coding professionals under- or over-code facet blocks because of the odd number of nerves to vertebra that occur in the cervical spine.
Let us review the spinal anatomy you will need to know for correct code selection. There are four regions of the spine: cervical, thoracic, lumbar, and sacral/coccyx. Each region contains numbered vertebrae and numbered nerves.
Vertebra:
- Cervical 1-7
- Thoracic 1-12
- Lumbar 1-5
- Sacral 1-5/Coccyx 1-4
Nerves:
- Cervical 1-8
- Thoracic 1-12
- Lumbar 1-5
- Sacral 1-5/Coccyx 1
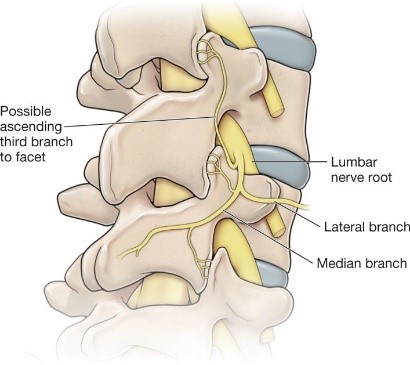
The facet joint is a synovial joint located between the superior articular process of one vertebra and the inferior articular process of the vertebra directly above it.
Facet joints are also referred to as zygapophyseal joints and Z-joints, so watch for these alternative terms in the documentation. Each facet joint is innervated by two spinal nerves.
{kind=link}
{kind=link}
Source: https://aneskey.com/radiofrequency-neurolysis/
As there is one more cervical nerve than there are vertebrae, the level listed will no longer match up perfectly starting with the C7-T1 facet joint. Because of the “extra” C8 nerve, all the nerves of the thoracic, lumbar, and sacral/coccygeal regions are innervated by the nerve above and below the facet joint. For example, L4-5 is innervated by “L3, L4” not “L4, L5.”
CPT Code Selection
There are up to three CPT® codes used to report facet joint injections based on spinal region. The codes allow for three levels maximum per session. Anything over three will not be reimbursed.
Cervical/Thoracic Facet Joints:
- 64490 Single (first) facet joint level
- 64491 Second facet joint level
- 64492 Third and all remaining facet joint levels (only bill once for all remaining levels 3+)
Lumbar/Sacral Facet Joints:
- 64493 Single (first) facet joint level
- 64494 Second facet joint level
- 64495 Third and all remaining facet joint levels (only bill once for all remaining levels 3+)
Billing and Coding Guidelines for Facet Joint Injection:
Each CPT code listed may be billed with a modifier 50 when injecting a level bilaterally. For one level unilateral or bilateral CPT, codes 64490 or 64493 should be used. If the facet joint injection is performed at more than one level, unilateral or bilateral CPT codes 64491, 64492, 64494, or 64495 should be used for the additional levels.
Fluoroscopic and CT guidance and localization for needle placement is included in codes 64490-64495.
If the injection is made around or into the spinal nerve, the service should be billed as a paravertebral nerve injection.
When destruction of the facet joint nerve is performed following the facet block, only the codes for the nerve destruction should be billed since their fee includes that of the facet nerve block procedure.
Best Practices
The OIG recovers billions of dollars every year from healthcare fraud schemes. This year alone has resulted in over 900 exclusions worth $1.5 billion. This highlights how seriously the OIG takes its work to detect and prevent fraud, waste, and abuse in health programs and operations.
Failing to not only implement best practices but properly detect and prevent fraud from occurring has severe consequences for providers. When healthcare providers are faced with an OIG investigation, it is crucial to understand enforcement actions to better know how to proceed.
Reasons for OIG Enforcements
OIG enforcements typically occur due to one of the following reasons:
- When an OIG analyst flags unusual practices or patterns
- When a whistleblower files a formal report
- When a patient reports their provider or files a formal complaint
It is always better to prevent instead of cure. To better protect themselves in an OIG investigation, healthcare programs should implement the following:
- Be complaint with coding and billing and have internal audits on at least a quarterly basis.
- Continuously review, update, and assess your internal compliance programs.
- Stay up to date on Medicare and other regulatory policies.
- Log in the OIG website frequently and review new items that are added to its active work plan. Also, sign up to receive the OIG email newsletter, which sends updates regarding completed OIG investigations and key changes to the OIG Work Plan.
- Develop robust internal coding, documentation, and medical necessity audit programs. Analyze the error trends from these audits and educate the appropriate revenue cycle management staff on how and why to prevent these errors including coding professionals, CDI staff, and physicians.
- Be proactive and perform reaudits if necessary based on error findings and upcoming OIG Work Plan updates.
Upcoming OIG Work Plan Audits on the Horizon
- Audits of Medicare Part B Laboratory Services During the COVID-19 Pandemic
- Yearend Review of Opioid Use in Medicare Part D in 2020
- Medicare Part D Payments During Covered Part A SNF Stay
- Audits of COVID-19 Telehealth Billing
As noted earlier, please continue to visit the OIG website for a complete listing of all active OIG Work Plan items.
Notes
- 2021 AMA CPT® Professional Edition Code Book
- American Society for Parenteral and Enteral Nutrition. May 2, 2021. “Office of Inspector General Report on Hospital Inpatient Billing for Severe Malnutrition.” https://aspen.informz.net/informzdataservice/onlineversion/pub/bWFpbGluZ0luc3RhbmNlSWQ9OTUzNzk4MA
- CMS (Centers for Medicare and Medicaid Services). 2014. Pub 100-04 Medicare Claims Processing. https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R2997CP.pdf
- Hendershot Cowart P.C. July 16, 2020. How to Protect Yourself in an OIG Enforcement. https://www.hchlawyers.com/blog/2020/july/how-to-protect-yourself-in-an-oig-enforcement/
- HR 748. 2020. Coronavirus Aid, Relief, and Economic Security Act, or the CARES Act. https://www.congress.gov/116/bills/hr748/BILLS-116hr748enr.pdf
- US Office of Inspector General. 2021. Review of Medicare Facet Joint Procedures. https://www.oig.hhs.gov/reports-and-publications/workplan/summary/wp-summary-0000400.asp
- US Office of Inspector General. 2021. Medicare Hospital Payments for Claims Involving the Acute- and Post-Acute-Care Transfer Policies. https://oig.hhs.gov/reports-and-publications/workplan/summary/wp-summary-0000445.asp
- US Office of Inspector General. 2020. Medicare Critical Care Services Provider Compliance Audit: Clinical Practices of the University of Pennsylvania. https://oig.hhs.gov/oas/reports/region3/31800003.asp
- US Office of Inspector General. 2020. Semiannual Report to Congress. https://oig.hhs.gov/reports-and-publications/archives/semiannual/2020/2020-fall-sar.pdf
- US Office of Inspector General. 2021. Physicians Billing for Critical Care Evaluation and Management Services. https://oig.hhs.gov/reports-and-publications/workplan/summary/wp-summary-0000316.asp
- US Office of Inspector General. 2021. Active Work Plan Items.https://oig.hhs.gov/reports-and-publications/workplan/active-item-table.asp
- US Office of Inspector General. 2021. Noridian Healthcare Solutions LLC Made Improper Medicare Payments of $4 Million to Physicians in Jurisdiction E for Spinal Facet-Joint Injections. https://www.oig.hhs.gov/oas/reports/region9/92003010.pdf
- US Office of Inspector General. 2021. Medicare Improperly Paid Acute-Care Hospitals $54.4 Million for Inpatient Claims Subject to the Post-Acute-Care Transfer Policy. https://oig.hhs.gov/oas/reports/region9/91903007.pdf
- US Office of Inspector General. 2020. Medicare Improperly Paid Physicians for More Than Five Spinal Facet-Joint Injection Sessions During a Rolling 12-Month Period. https://oig.hhs.gov/oas/reports/region9/92003003.asp
- US Office of Inspector General. 2020. Hospitals Overbilled Medicare $1 Billion by Incorrectly Assigning Severe Malnutrition Diagnosis Codes to Inpatient Hospital Claims. https://oig.hhs.gov/oas/reports/region3/31700010.asp
Leigh Poland, RHIA, CCS (leigh.poland@agshealth.com) is the executive director of education at AGS Health.
Srivalli Hariharamuthukrishnan, CPC (srivalli.harihara@agshealth.com) is the senior manager of coding education at AGS Health.