Why Electronic Case Reporting Is Vital During Pandemics
According to the Centers for Disease Control and Prevention (CDC), electronic case reporting (eCR) is the “automated generation and transmission of case reports from an electronic health record (EHR) to public health agencies for review and action. eCR makes disease reporting from healthcare providers to public health faster and easier.”1
Reporting of cases or diseases provides an understanding of occurrences and trends that assists with public health planning efforts, resource allocation, and policymaking. Typically, case reporting, which is required by law to report to state and local public health entities regarding specific diseases and conditions, has been conducted via paper-based methods. Paper-based methods cause several challenges in public health’s ability to report timely data that supports their efforts in conducting regular surveillance to help prevent, investigate, report, and control disease outbreaks.
Passage of the Health Information Technology for Economic and Clinical Health Act (HITECH Act), enacted under the American Recovery and Reinvestment Act of 2009 (ARRA), served as a catalyst for adopting, implementing, and using health information technologies (health IT) and transitioning away from paper-based reporting to a more advanced process of eCR. The Centers for Medicare and Medicaid Services (CMS) Meaningful Use EHR Incentive Program issued a final rule in 2015 for Stage 3 that added eCR as a new public health measure.
Enacting this law created unprecedented opportunities for public health agencies and facilitated a much-needed push toward electronic reporting. However, the ability for public health agencies to receive electronic reporting information was still nascent and progress was slow in this area. Without laying the framework through policy levers and making eCR a requirement, public health agencies have been slow to adopt as the infrastructure and funding make this a lower priority.
Despite these challenges, EHRs and other health IT solutions have advanced stakeholders’ ability to collect, analyze, and report on required public health surveillance efforts. As these technologies have matured since HITECH, health information exchanges (HIEs) and other case reporting systems have emerged to support eCR and have become more widely adopted. eCR provides several benefits over paper-based reporting, such as:
- Reduces response time by automatically submitting required case reporting to designated public health agencies
- Reduces manual entry, faxing, and phone calls
- Complies with reporting requirements for the Promoting Interoperability Program (formerly meaningful use) for implementing eCR
- Complies with HIPAA and state reporting laws
- Monitors the spread of reportable conditions such as COVID-19
Although eCR provides many benefits to stakeholders as they transition away from paper-based reporting, public heath reporting systems remain fragmented and siloed. This has created significant challenges, and with the onset of COVID-19, it has exposed limitations within the United States’ public health surveillance system in a significant way where timeliness, completeness, and accuracy of data is critical in the pandemic’s response efforts.
Congressional Efforts Supporting COVID-19 Response
To support public health agencies and their ability to report data in response to COVID-19, Congress has taken several steps. The Coronavirus Aid, Relief, and Economic Security Act (CARES Act) that was signed into law in March 2020 provided a $2.2 trillion economic stimulus, which included $500 million for the CDC to support “public health data surveillance and analytics infrastructure modernization.”2 In supplemental appropriations for COVID-19, the CDC has received $7.5 billion and $10.25 billion in grants for testing and other public health purposes (including surveillance). Additional funding may be transferred to the CDC from other US Department of Health & Human Services (HHS) accounts and used by the agency for surveillance purposes.
Lab Reporting Requirements
The CARES Act requires that every clinical laboratory that performs or analyzes tests—which are intended to detect or diagnose possible cases of COVID-19—to report the results to HHS. The reporting period and format of the data submission is at the discretion of the HHS secretary until the end of the COVID-19 Public Health Emergency declaration or any extension that has been granted.
Congressional Reports
The Paycheck Protection Program and Health Care Enhancement Act (PPPHCEA), enacted in April 2020, required analyses and reporting of COVID-19 data by HHS. Congress required no later than 21 days after enactment, and every 30 days until the end of COVID-19 PHSA, HHS was required to report on testing, cases, hospitalizations, and death, which also included de-identified demographic data and other relevant factors. Congress also expected HHS to report on, no later than 180 days after enactment, the number of positive diagnosis, hospitalizations, and deaths as a result of COVID-19 and any other factors.
eCR Now
As COVID-19 emerged and persisted across the country (and the world), it became clear that a solution was needed quickly to address the rapidly spreading disease. Relying on the currently mostly paper-based and inconsistent infrastructure was insufficient to provide a rapid response to the evolving health crisis.
Despite policy and funding efforts within Promoting Interoperability, eCR was in the early deployment stages and existed only in a limited number of sites led by the CDC, the Council of State and Territorial Epidemiologists, and the Association of Public Health Laboratories (APHL) when COVID-19 was first identified.
Seeing an urgent need to address the rapidly developing public health crisis, the eCR team developed a strategy, termed eCR Now, for immediate deployment. eCR Now provides the identifiable clinical patient data as required to state and local public health agencies that are needed to support outbreak management and action.
According to John W. Loonsk, MD, FACMI Adjunct Associate Professor, Johns Hopkins Bloomberg School of Public Health, Consulting Chief Medical Informatics Officer, Association of Public Health Laboratories since the beginning of COVID-19 more than 6,900 facilities have reported on COVID-19 through eCR.
eCR supports three different approaches toward reporting COVID-19 cases:
Element 1: A cohort based COVID-19 rapid eCR implementations for sites that have eCR-enabled EHRs. This approach leverages the FHIR trigger code distribution service that allows users to stay current with codes (ICD-10, LOINC, SNOMED) as they change. Confirmed cases reported to public health agencies are not required to submit data via manual entry and reporting, thus reducing the burden on providers and public health.
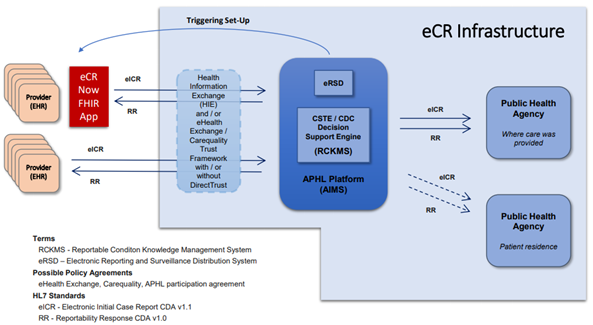
Element 2: eCR Now FHIR SMART App (as shown in Figure 1) is a solution supporting EHRs that are non-eCR enabled to ramp up quickly for reporting purposes. This app connects the COVID-19 eCR to existing infrastructure and automatically reports triggering and trigger codes, electronic initial case reporting (eICR), reportability response sorting, etc., through the APHL Informatics Messaging Services (AIMS) shared services infrastructure. Different implementation models are provided to support different options, such as local or cloud hosting, SMART on FHIR or through a system application launch. Figure 1 demonstrates the infrastructure of eCR Now and how the app is integrated into the current reporting workflow.3
Figure 1: eCR Infrastructure
{kind=link}
Element 3: A nationwide eCR trust framework for eHealth Exchange, Carequality, CommonWell members, and those entities that connect with them to support the onboarding process. Participants that currently conduct eCR are not required to develop new legal agreements for their participation.
CDC’s Data Modernization Initiative
At the urging of key stakeholders and support from the CDC director and Congress, in 2014 the CDC began its journey toward a modernized surveillance strategy that allows the agency to move toward anticipating threats rather than reacting to them. The plan highlighted three goals: 1) enhance the workforce; 2) accelerate the use of emerging tools and approaches to improve the availability of quality and timely surveillance data; and 3) demonstrate early successes through four crosscutting surveillance system initiatives (mortality reporting, case reporting, electronic laboratory reporting, and syndromic surveillance) to improve public health surveillance outcomes. Since then, the CDC made progress in its modernization efforts and had begun to pilot new systems for data sharing between public health departments and healthcare organizations in real time through the Digital Bridge initiative. In fiscal year 2020, Congress provided its first specific appropriations ($50 million) to the CDC for “Public Health Data Surveillance/IT Systems Modernization.” In previous years, the CDC’s modernization efforts were funded through other budget line items.
By the time the pandemic arrived, public health reporting was still reliant on siloed, manual, and paper-based processes to exchange or report data. Meeting the volume and velocity of reporting needs for COVID-19 overwhelmed public health data systems and their infrastructure, which created challenges for reporting. The CARES Act provided the CDC with $500 million for data surveillance and analytical infrastructure that will boost its efforts in modernizing public health data and reporting initiatives for immediate COVID-19 needs and for the long-term. With this funding, the CDC expects to:
- Leverage data for surveillance, detection, and improving jurisdictions’ situational awareness to allow localized, targeted responses and decision-making using more real-time data to respond to outbreaks like COVID-19.
- Expand the electronic exchange and integration of information between public health and healthcare, including electronic health records, which is essential for timely, accurate, and accessible disease surveillance.
- Support for public health’s data science, informatics, and IT workforce; expanding core data, informatics, and IT capacity; advancing interoperable systems and tools; strengthening and expanding collaboration.4
The CDC has expanded its automated reporting for COVID-19 test results from laboratories to health departments and the CDC, with 46 jurisdiction having converted to electronic systems as of October 16, 2020.5 New investments in fiscal year 2020 through CARES Act supplemental funding enabled the CDC to begin strengthening the public health data and surveillance infrastructure of the US through the launch of the agency wide Public Health Data Modernization Initiative (DMI).
The CDC is also collaborating with the eCR Now initiative to implement eCR that will enable data exchange between public health agencies and healthcare providers. Finally, as the Office of the National Coordinator for Health IT (ONC) is preparing its interoperability rules for EHRs in 2022, the CDC is working with the agency to support its attempts at public health data modernization.
COVID-19 has demonstrated the need for a strong public health infrastructure that is capable of electronically collecting and reporting on data to federal, state, local, and tribal communities. It has also brought to light the challenges of getting the right information to the right people at the right time when needed most.
Once health emergencies occur, especially public health emergencies the size and scope of COVID-19, you may believe that is not the time to advance programs in their nascent stages such as eCR Now or the CDC DMI, but it is exactly that time when our focus is on public health data reporting from a policy, planning, financial, and resource perspective when it is needed most.
Notes
- Centers for Disease Control and Prevention (CDC). “eCR Now: COVID-19 Electronic Case Reporting.” cdc.gov/coronavirus/2019-ncov/php/electronic-case-reporting.html
- Congressional Research Service. “Tracking COVID-19: U.S. Public Health Surveillance and Data.” November 20, 2020.
- Electronic Case Reporting. eCR General Information. https://ecr.aimsplatform.org/general/ecr-now-covid-19-fhir-app-challenge.
- Centers for Disease Control and Prevention (CDC). “CDC Public Health Data Modernization.” cdc.gov/budget/documents/fy2021/fy2021-PHDM-factsheet.pdf.
- Congressional Research Service.
Taking the Pulse of the Nation’s Social and Mental Wellness
Wanting to acquire information and understand the impact on economic and mental health of American households as a result of COVID-19, the National Center for Health Statistics partnered with the US Census Bureau and several other agencies to develop an experimental data system called the “Household Pulse Survey.”
The program consists of three phases, with phase one focusing on employment status, food security, housing, access to healthcare, educational disruption, and physical and mental health. The data collected will help to uncover what people are experiencing during the pandemic.
Because this initiative is a first of its kind, the federal statisticians are keeping an eye on the quality of the data to ensure data that is reported remains high.
Author’s Note: This citation belongs to the Household Pulse Survey. “Novel COVID-19 survey takes nation’s social, mental ‘Pulse.”
Allison Viola (aviola@guidehouse.com) is director at Guidehouse.