Measuring Coding Accuracy and Productivity in Today’s Value-Based Payment World [Sponsored]
By Kim Charland, BA, RHIT, CCS
Much has been written over the past two years on ICD-10-CM/PCS coding accuracy and productivity. Analysis has included the comparison of coding accuracy between ICD-9 and ICD-10 with the same 95 percent accuracy goal set. Is this really achievable only two years into a new coding system? How long did it take to achieve 95 percent accuracy in ICD-9? I believe that many in our industry are still basing coding accuracy and productivity on historical “transaction” type coding—principal diagnoses, secondary diagnoses to include MCCs and CCs for optimized DRG, present on admission (POA), principal, and secondary procedures.
Transactional versus Relational Coding
Today we must ask ourselves, “Is coding still transactional or is it more “relational?” MacMillan defines the term “relational” as “relating to the relationship or connection between two or more things.” Another definition that speaks to being relational is how we interact with others. So what does “relational” have to do with coding? Everything.In the United States, diagnosis and procedure codes have been used primarily to collect data for organizations such as the World Health Organization and for fee-for-service reimbursement—DRG, APC, Physician Fee Schedule, etc. However, in recent years, coded data has become “relational” to so much more, including:
- Reimbursement for quality of care, not just volume—such as HVBP, HRRP, HACs, MACRA
- Risk adjustment related to severity of illness (SOI), risk of mortality (ROM), hierarchical condition categories (HCCs)
- Quality scores and provider profiles
- Data mining for Regulatory Audit Focus such as OIG, RACs, and more
- Population health management initiatives
- Payer contract negotiations
- Bundled payment preparation
Coding Contest Reveals Decreased Accuracy, Increased Productivity
So what is a realistic coding accuracy rate in ICD-10? The Central Learning 2nd National ICD-10 Coding Contest findings reveal coding accuracy rates far below the 95 percent accuracy standard.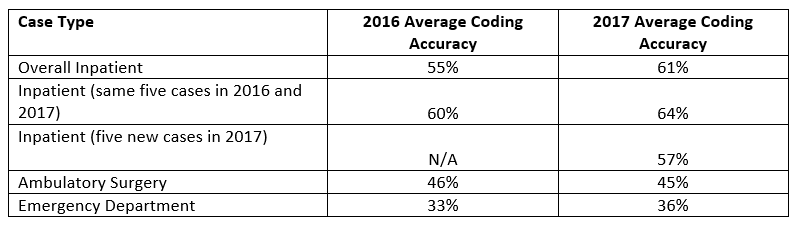{kind=link}
Diagnosis chapters with the lowest code accuracy included:
- Congenital malformation, deformations, and chromosomal abnormalities (Q00-Q99)
- Diseases of the skin and subcutaneous tissue (L00-L99)
- Certain infectious and parasitic diseases (A00-B99)
- Diseases of the nervous system (G00-G99)
- Diseases of the genitourinary system (N00-N99)
{kind=link}
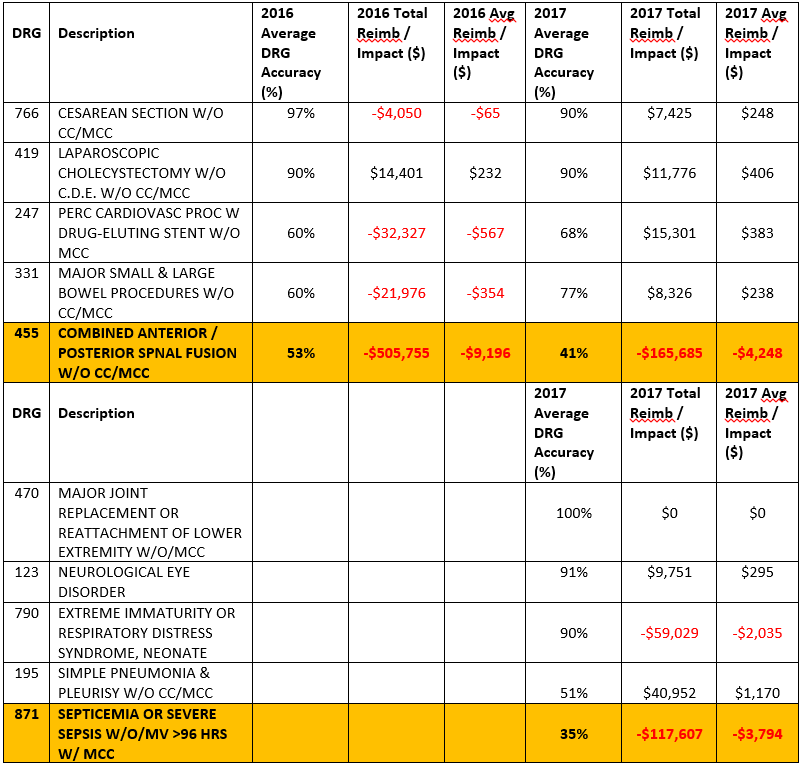
The DRG detail is provided in the table below:
{kind=link}
In addition, and not surprising, coding accuracy for participants decreased as productivity increased:
- Coding productivity per hour: inpatient cases 2.5/outpatient cases 4.8
- Higher productivity decreased inpatient coding accuracy by -25.4 percent
- Higher productivity decreased outpatient coding accuracy by -20.3 percent
Audit Focus Shifts to Quality and Integrity
Recent conversations with health information management (HIM) professionals have revealed insights on ICD-10 coding accuracy, productivity, and the focus of their coding audits (reimbursement vs. quality). It was alarming to hear how many of their audits are driven by finance and remain focused mainly on reimbursement, based on the belief that coding is still transactional. However, a few have started focusing on relational types of coding audits—how coding impacts severity of illness, risk adjustment, quality reporting, data mining by payers, and government auditing programs.These HIM professionals are actually performing different types of audits based on what they want to assess. Though some are still reimbursement-focused to ensure sufficient cash flow, many are focusing on documentation integrity, quality, and risk adjustment. They are seeing how coding relates to clinical documentation improvement and quality. Ensuring that medical record documentation is complete and coding is accurate relates to quality reporting requirements for value-based reimbursement.
Ten Tips to Help Prepare for 2018 Audits
As you prepare your auditing budgets for 2018, here are some thoughts to keep in mind:- Don’t forget the reimbursement audit and run your data on your top 10‐20 paying DRGs for the first two quarters of 2018, especially since the 2018 IPPS changes went into effect October 1.
- Be sure your finance team and revenue cycle team are aware of the impending CMI impact from 2018 changes.
- Continue to audit your procedure coding for accuracy and opportunity, given the challenges of ICD-10-PC coding.
- Begin to perform coding assessments that include SOI, ROM, and HCCs and evaluate the potential value-based payment risk-adjust impact.
- Continue assessing coder knowledge in ICD-10 and CPT coding.
- Provide targeted ICD-10 education and training to address knowledge gaps.
- Supplement internal coding reviews with external coding audits.
- Balance coding productivity and accuracy performance metrics.
- Monitor coding denials from payers.
- Continue to educate your team—CDI, coding, quality, and physicians.
Kim Charland (kim.charland@pena4.com) is the Vice President of Strategic Initiatives for Pena4 and the President of the New York Health Information Management Association.
H.I.M. ON CALL is now Pena4, a health information solutions company dedicated to improving mid-cycle performance. We are your single, proven source for coding, auditing, consulting, clinical revenue and business process management services.